OK. #SK COVID-19 mega-thread.
NEW #SK Omicron models (via @DennisKendel) Jan 19:
- Measures implemented to SIGNIFICANTLY reduce social mixing, MAYBE we avoid disaster/triage in #SK hospitals.
- Do NOTHING, #SK hospitals crushed, triage ensues.
Get comfy - here we go.
(1/25)
NEW #SK Omicron models (via @DennisKendel) Jan 19:
- Measures implemented to SIGNIFICANTLY reduce social mixing, MAYBE we avoid disaster/triage in #SK hospitals.
- Do NOTHING, #SK hospitals crushed, triage ensues.
Get comfy - here we go.
(1/25)

Let's begin with history.
@SKGov was provided w/ models from WORLD-CLASS #SK modeler Dr. Nate Osgood in late August 2021 that predicted EXACTLY how #SK ICUs would be overwhelmed w/ Delta in Fall 2021.
Nothing was done. Everything left wide open.
(2/n)
thestarphoenix.com/news/local-new…
@SKGov was provided w/ models from WORLD-CLASS #SK modeler Dr. Nate Osgood in late August 2021 that predicted EXACTLY how #SK ICUs would be overwhelmed w/ Delta in Fall 2021.
Nothing was done. Everything left wide open.
(2/n)
thestarphoenix.com/news/local-new…
Also August 2021, consensus letter sent by #SK MHOs (led by @CoryNeudorf) to @SKGov recommends NUMEROUS measures to stem Delta:
Universal indoor masks, proof of vaccine, gathering/capacity limits, increased contact tracing capacity.
Nothing.
(3/25)
Universal indoor masks, proof of vaccine, gathering/capacity limits, increased contact tracing capacity.
Nothing.
(3/25)
https://twitter.com/awong37/status/1434878935645499399
Delta surges. @SKGov implements indoor mask mandates Sept 16, LAST province in Canada to do so. Proof of vaccine mandates announced for Oct 1.
Mandates had been left to businesses, organizations, football teams (!), school divisions. Mass chaos.
(4/25)
cbc.ca/news/canada/sa…
Mandates had been left to businesses, organizations, football teams (!), school divisions. Mass chaos.
(4/25)
cbc.ca/news/canada/sa…
On Oct 18, @SaskHealth begins transferring critically ill #SK pts to Ontario to relieve overwhelmed #SK ICUs.
Transfers cancelled, restarted. Clinical, communications, PR DISASTER.
In the end, 27 #SK pts transferred. 6 die in #ON. Devastating.
(5/25)
cbc.ca/news/canada/sa…
Transfers cancelled, restarted. Clinical, communications, PR DISASTER.
In the end, 27 #SK pts transferred. 6 die in #ON. Devastating.
(5/25)
cbc.ca/news/canada/sa…
*348* #SK citizens die of #COVID19 during #SK's Delta surge (Sep 1 - Dec 31).
Comparatively, that's *4350* people dead in #ON!
Not all deaths preventable, but MANY could have been with good policy.
MODELLING was RIGHT THERE. Yet, no action.
(6/25)
Comparatively, that's *4350* people dead in #ON!
Not all deaths preventable, but MANY could have been with good policy.
MODELLING was RIGHT THERE. Yet, no action.
(6/25)
https://twitter.com/awong37/status/1455251044464795651
Now, amazingly, here we are again.
Dr. Osgood's WORLD-CLASS models say #SK hospitals & ICUs overwhelmed FOR SURE if no additional measures to limit social gatherings.
Yet, Premier Moe says Jan 18 measures "cause significant harm for no clear benefit".
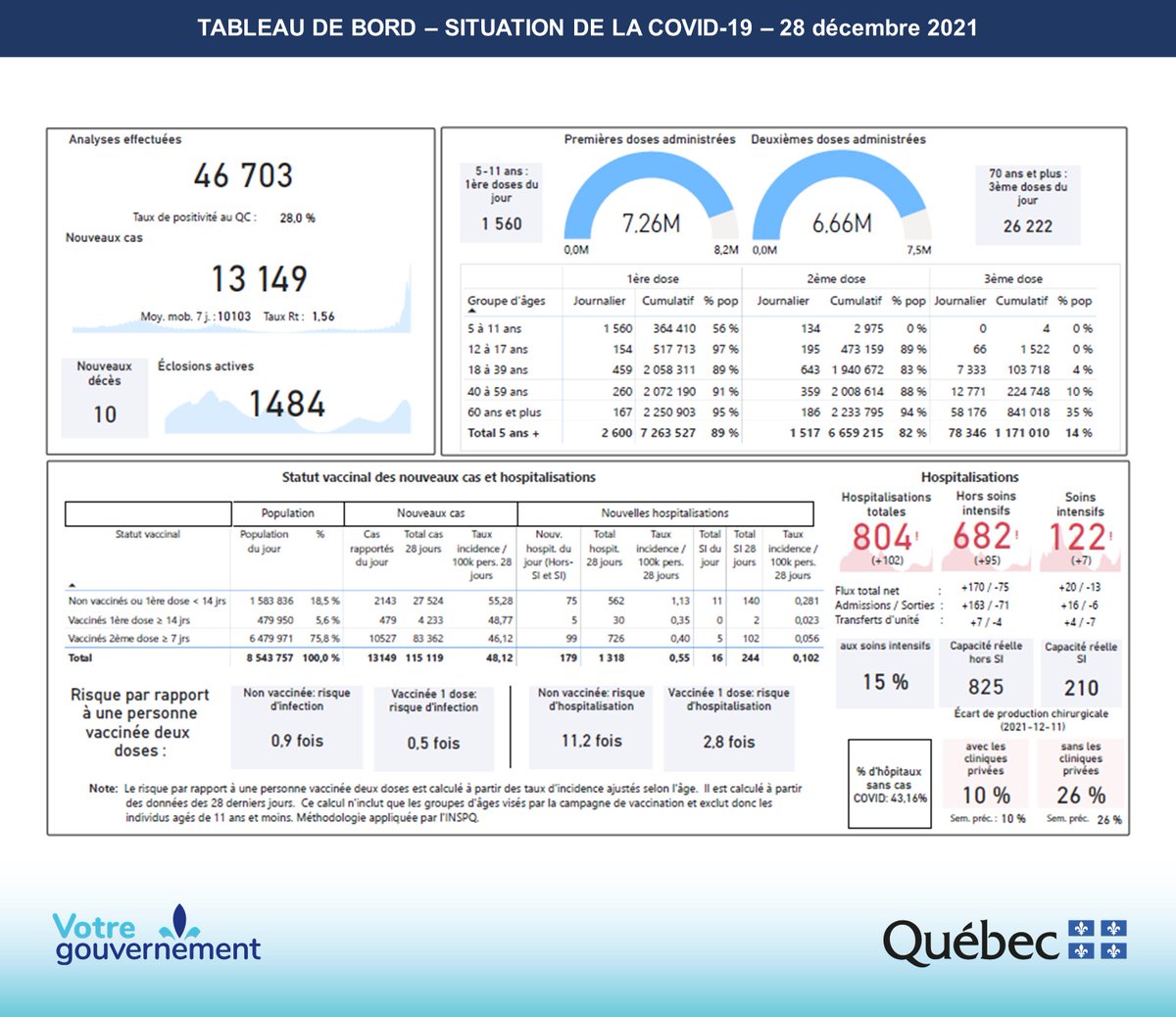
Cites #QC crisis.
(7/25)
Dr. Osgood's WORLD-CLASS models say #SK hospitals & ICUs overwhelmed FOR SURE if no additional measures to limit social gatherings.
Yet, Premier Moe says Jan 18 measures "cause significant harm for no clear benefit".
Cites #QC crisis.
(7/25)

Excellent thread @MoriartyLab. #QC reports deaths QUICKLY & ACCURATELY. Better than anyone else in Canada.
Hence, #SK death counts are likely huge UNDERESTIMATE.
If you're going to compare numbers, please know & EXPLAIN caveats of data.
(8/25)
Hence, #SK death counts are likely huge UNDERESTIMATE.
If you're going to compare numbers, please know & EXPLAIN caveats of data.
(8/25)
https://twitter.com/MoriartyLab/status/1483853182346440711
Also, was Premier Moe comparing #SK's death rates per capita vs. others during Delta's surge in Fall 2021 in any public forum?
No. Why?
Because #SK had WORST per capita death rates in Canada with Delta BY FAR.
~3X excess deaths in #SK vs Canada
(9/25)
ctvnews.ca/health/coronav…
No. Why?
Because #SK had WORST per capita death rates in Canada with Delta BY FAR.
~3X excess deaths in #SK vs Canada
(9/25)
ctvnews.ca/health/coronav…
In summary, @SKGov CHOSE to be MAJOR OUTLIER with Delta. #SK citizens pay a HEAVY price.
No measures except masks & proof of vaccine. Implemented those FAR TOO LATE.
ICUs overwhelmed. Triage occurs. #ON ICUs save us.
So much PREVENTABLE death & suffering.
(10/25)
No measures except masks & proof of vaccine. Implemented those FAR TOO LATE.
ICUs overwhelmed. Triage occurs. #ON ICUs save us.
So much PREVENTABLE death & suffering.
(10/25)
The Premier's approval ratings over management of #COVID19 continue to fall. Close to 60% disapprove of @SKGov decisions Jan 17.
Yet, @SKGov shows NO learning from past experience. They keep ignoring Dr. Shahab's advice.
"Carry on, #SK!"
(11/25)
cbc.ca/news/canada/sa…
Yet, @SKGov shows NO learning from past experience. They keep ignoring Dr. Shahab's advice.
"Carry on, #SK!"
(11/25)
cbc.ca/news/canada/sa…
Let's go back to new/updated Omicron modeling now and see the price of "carrying on" with NO additional measures put in place.
The models make it clear.
Here it is again for reference. Let's work through the various scenarios one-by-one.
(12/25)
The models make it clear.
Here it is again for reference. Let's work through the various scenarios one-by-one.
(12/25)
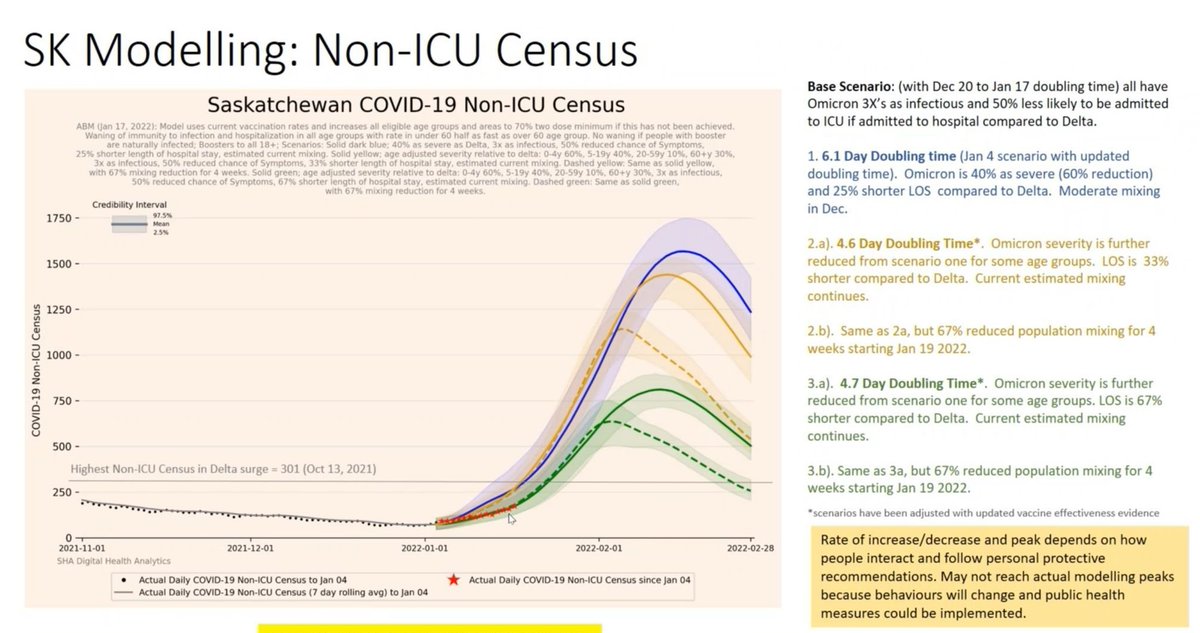
The blue line models with a 6.1 day doubling time (likely underestimate) for Omicron, and 60% "less severity" vs. Delta. No changes in social mixing.
Our Omicron wave is long, protracted, and painful. It peaks in late-Feb with over 1,500 admitted to hospital.
Horrible.
(13/25)
Our Omicron wave is long, protracted, and painful. It peaks in late-Feb with over 1,500 admitted to hospital.
Horrible.
(13/25)
The yellow lines model a 4.6 day doubling time (more reasonable) for Omicron, but also assumes even further lessened severity for certain age groups and decreased length of stays for those admitted to hospital.
Lots of assumptions there, many VERY optimistic.
(14/25)
Lots of assumptions there, many VERY optimistic.
(14/25)
Even WITH 'best case' assumptions, if no additional measures we peak in mid-Feb with nearly *1500* in hospital. Absolutely nuts.
*If* we put measures in place to reduce mixing by 2/3rds, curve IS significantly blunted. Peak early Feb, ~1,100 hospitalized. Still nuts.
(15/25)
*If* we put measures in place to reduce mixing by 2/3rds, curve IS significantly blunted. Peak early Feb, ~1,100 hospitalized. Still nuts.
(15/25)
The green lines are the MOST optimistic scenarios. 4.6 day doubling time, further lessened severity for Omicron for certain age groups, even further decreased lengths of stay for hospitalized patients.
Many assumptions. Likely FAR TOO optimistic, IMO.
(16/25)
Many assumptions. Likely FAR TOO optimistic, IMO.
(16/25)
Even WITH "best-case" assumptions, we peak in mid-Feb at ~750 in hospital. It drags, painfully, to end of Feb.
With additional measures to reduce mixing by 2/3rds, we peak early Feb at ~650 in hospital and come down fast.
*Maybe* we avoid triage if chips fall right.
(17/25)
With additional measures to reduce mixing by 2/3rds, we peak early Feb at ~650 in hospital and come down fast.
*Maybe* we avoid triage if chips fall right.
(17/25)
To be clear, NO scenario avoids cancellation of ALL "non-life-saving" procedures and surgeries again. That's INEVITABLE at this point.
EVERYONE who has been waiting months/years will be pushed down yet again.
Let's call it for what it is: MASS triage of #SK citizens.
(18/25)
EVERYONE who has been waiting months/years will be pushed down yet again.
Let's call it for what it is: MASS triage of #SK citizens.
(18/25)
#SK is in a HORRIBLE place right now.
We have the LOWEST 1st/2nd dose uptake across all provinces except #AB.
We're the ONLY province with NO capacity/gathering limits.
Not even immunity from all our Delta recoveries will help, as Omicron's basically a new virus.
(19/25)
We have the LOWEST 1st/2nd dose uptake across all provinces except #AB.
We're the ONLY province with NO capacity/gathering limits.
Not even immunity from all our Delta recoveries will help, as Omicron's basically a new virus.
(19/25)
Worst of all, @SKGov REFUSES to acknowledge impending #Omicron surge.
Do they REALLY believe it's not going to happen?
They publicly say Saskatchewan will be fine, they're "monitoring the situation". They continue to gaslight the electorate:
"We're good, no sweat."
(20/25)
Do they REALLY believe it's not going to happen?
They publicly say Saskatchewan will be fine, they're "monitoring the situation". They continue to gaslight the electorate:
"We're good, no sweat."
(20/25)
Dr. Shahab issues CLEAR instructions. DON'T GATHER unless for work/school.
Premier Moe? No measures needed. They're "not helpful". They're "damaging".
When the Premier is asked who #SK public should trust?
"They should trust themselves."
🙄🧐
(21/25)
cbc.ca/news/canada/sa…
Premier Moe? No measures needed. They're "not helpful". They're "damaging".
When the Premier is asked who #SK public should trust?
"They should trust themselves."
🙄🧐
(21/25)
cbc.ca/news/canada/sa…
Since @SKGov is monitoring the situation, they'll see that cases / hospitalizations are all surging, as we would expect. Here's Jan 19 data.
Hospitalizations are following the EXACT timeline as predicted by Dr. Osgood's modeling
It's all there, in plain sight.
(22/25)
Hospitalizations are following the EXACT timeline as predicted by Dr. Osgood's modeling
It's all there, in plain sight.
(22/25)

So we'll see, THIS WEEK, whether @SKGov chooses to put additional measures in place to give #SK hospitals a fighting chance.
If they do nothing, that's implicit endorsement they're *OK* with letting #SKs smoldering healthcare system burn down yet again.
#SK HCWs? 😢😢
(23/25)
If they do nothing, that's implicit endorsement they're *OK* with letting #SKs smoldering healthcare system burn down yet again.
#SK HCWs? 😢😢
(23/25)
Letting COVID run unchecked as @SKGov has, sacrifices the health of ALL #SK citizens, destroys the publicly-funded healthcare system, and results in immeasurable health consequences (kids!! the vulnerable!!), suffering, & deaths.
It's complete misery. So preventable.
(24/25)
It's complete misery. So preventable.
(24/25)
It ISN'T too late for CRITICAL policy measures to save #SK hospitals.
NOT LOCKDOWN. Appropriate measures. ASAP.
PLEASE, stop pretending, blaming, gaslighting.
PLEASE, lead. Show courage & integrity. CARE about the lives of your electorate.
We CAN do it. TOGETHER.
(/end)
NOT LOCKDOWN. Appropriate measures. ASAP.
PLEASE, stop pretending, blaming, gaslighting.
PLEASE, lead. Show courage & integrity. CARE about the lives of your electorate.
We CAN do it. TOGETHER.
(/end)
• • •
Missing some Tweet in this thread? You can try to
force a refresh